
Mastitis what is it? And how should it be treated?
In the last week I have worked with two mums with mastitis, both with very different causes and symptoms. I will come back to them, but first, what is mastitis?
The word mastitis originates from medical Latin, combining the Greek ‘masto’ (breast) and ‘itis’ (swelling) to mean "inflammation of the breast" This is a pretty accurate description of what it is and it can be a relatively common occurrence for breastfeeding women. It can range from early postpartum engorgement, a distinct condition that shares some clinical features with mastitis and those characterised by localised swelling (normally in one breast), discolouration of the skin, including shiny taut and hot areas and in extreme cases, if untreated, an abscess. Mastitis is also associated with a range of distinctive symptoms from sore and achey to extreme pain and experiencing high fever, chills and tachycardia.
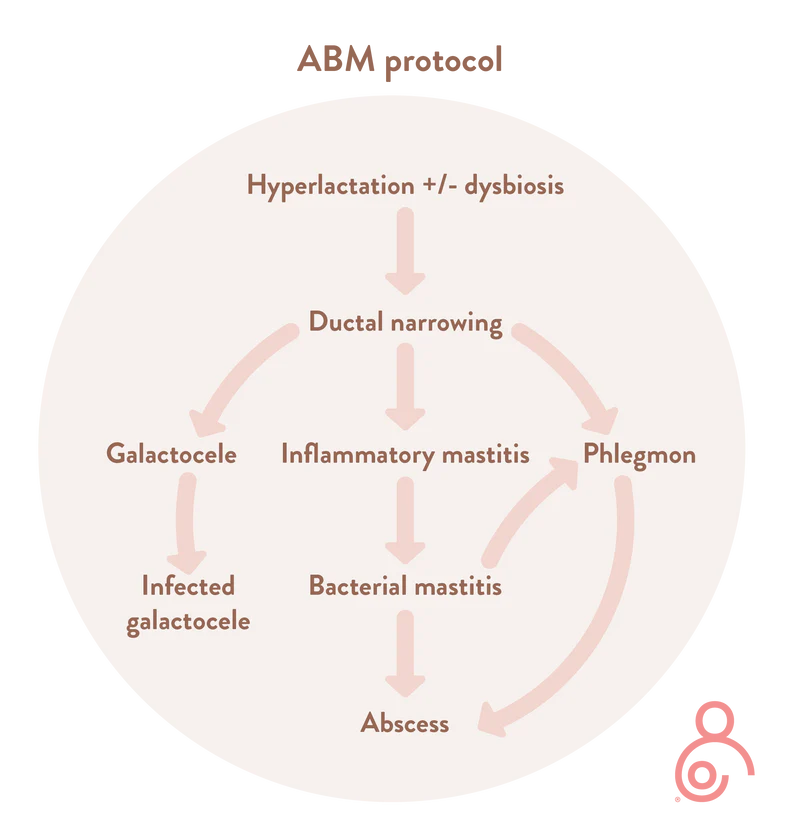
In the past, mastitis was thought of as a single pathological entity in the lactating breast. However, new evidence demonstrates that mastitis encompasses a spectrum of conditionsthat result from ductal inflammation and stromal edema. In the revised ABM protocol they say:
‘If ductal narrowing and alveolar congestion are worsened by overstimulation of milk production, then inflammatory mastitis can develop, and acute bacterial mastitis may follow. This can progress to phlegmon or abscess, particularly in the setting of tissue trauma from ag- gressive breast massage. Galactoceles, which can result from unresolved hyperlactation, can become infected. Subacute mastitis occurs in the setting of chronic mammary dysbiosis, with bacterial biofilms narrowing ductal lumens’.
Credit: https://lactamo.com/
Dr Pamela Douglas Re-thinking benign inflammation of the lactating breast: Classification, prevention, and management - PubMed proposed a model of breast inflammation ‘in which very high intra-alveolar and intra-ductal pressures are hypothesised. It is thought that this pressure puts strain on, or ruptures the tight junctions between lactocytes and ductal epithelial cells, triggering inflammatory cascades and capillary dilation. The increase in stromal tension leads to pressure on lactiferous ducts, resulting in a worsening of intraluminal backpressure. Rising leucocyte and epithelial cell counts in the milk and alterations in the milk microbiome are signs that the mammary immune system is recruiting mechanisms to downregulate inflammatory feedback loops leading to potential pain and oedema which can then worsen the ductal pressure’.
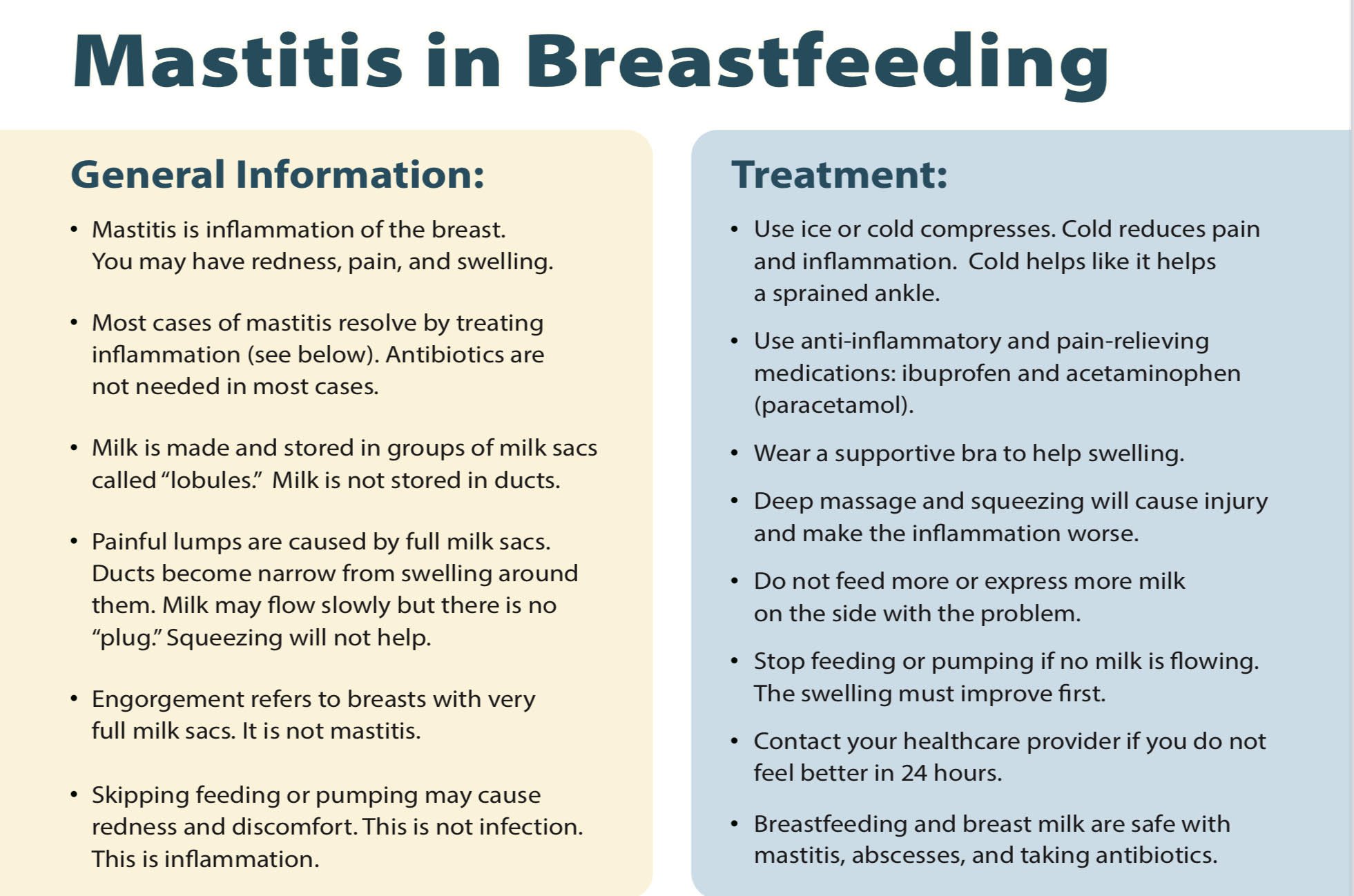
So, with inflammatory mastitis, breast inflammation is understood to be due to the body’s reaction to a build up of breast milk. It is thought that when breasts are very full pressure is placed on the milk ducts which can then trigger a systemic inflammatory response (SIRS) This type of inflammation creates a significant and rapid whole body response but it doesn’t mean it is infective.
Dr Katerina Mitchel, a breast surgeon and IBCLC says ‘Mastitis the vast majority of the time is inflammatory rather than infectious. It is often caused by hyperlactation (oversupply) and/or transient engorgement of a region of breast tissue. Full “milk sacs” (i.e. alveolar cells) can be painful and lumpy. In addition, a lot of blood flow in the area makes the area red and swollen.
This understanding comes with new ways to manage mastitis, it doesn’t necessarily need to be treated with antibiotics. In fact, Dr Naomi Dow a breastfeeding medicine GP and IBCLC , says she rarely prescribes them anymore. Although I am not licensed to prescribe medication, I can share current evidence based protocols on treating mastitis and help to find the root cause. I have seen so many of my clients benefitting from this and it makes a lot of sense to me. Inflammatory mastitis often resolves without antibiotic treatment, and antibiotic use can lead to dysbiosis, a further risk factor for recurrent mastitis.
So what does this all mean?
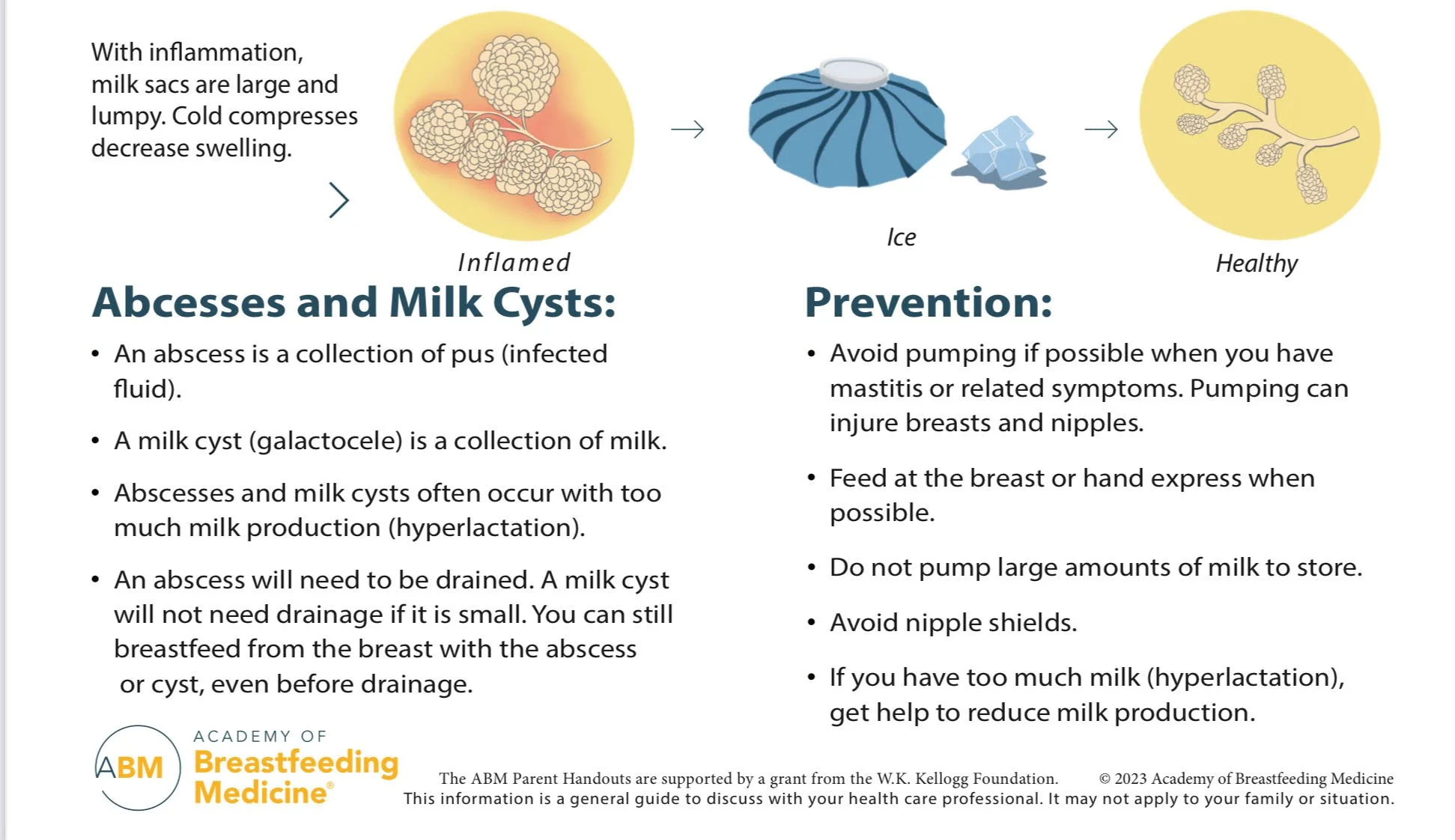
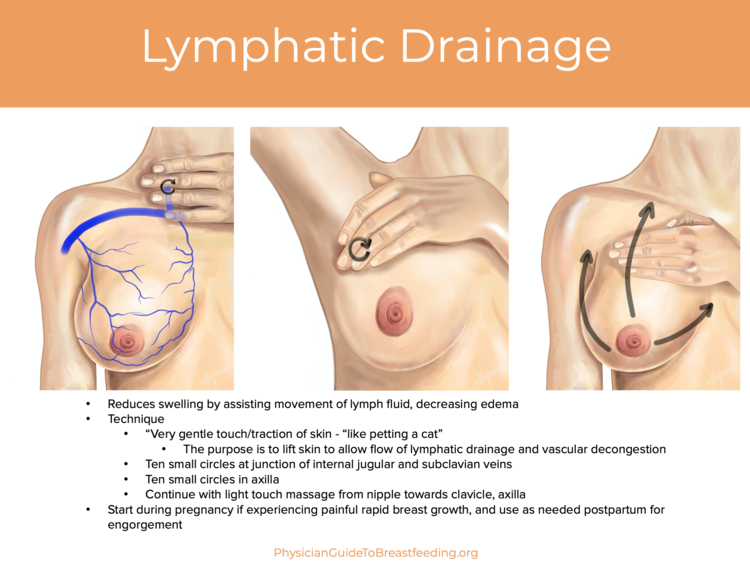
The old guidelines were to remove as much milk as possible along with using hot compresses and firm massage towards the nipple. Our new understanding recommends, applying ice packs to the affected area for 10 mins every hour during the day, no extra milk removal, no firm massage but very gentle lymph drainage techniques towards the armpit along with appropriate anti inflammatory medication.
Credit: https://www.bfmed.org/
Inflammatory Mastitis symptoms often clear on their own after a day or two of careful preventative treatment. However, If the progression of ducal narrowing and inflammation continues and a bacterial infection is present, it may need antibiotics and further treatment. Bacterial infections are not as common and are usually caused by staphylococcus (staph) or streptococcus (strep) or MRSA Staph, MRSA and Breastfeeding - Breastfeeding Support. An untreated bacterial infection can then progress to a firm breast mass or phlegmon and then on to an infected fluid collection, an abscess that will necessitate drainage. Approximately 3-11% of women that develop acute mastitis will go on to develop an abscess.
As the breast is highly vascular it seems clear to me that excessive heat, hard massage and expressing, especially with ill fitting flanges did a lot to cause tissue damage and further inflamation. Unfortunately, even though this new protocol by the ABM was written in 2022, I’m still hearing and seeing these techniques recommended.
So back to my clients. The first one developed severe bilateral mastitis on day 3, unfortunately she had developed sore and damaged nipples whilst in hospital and we found out after a milk culture that she had MRSA. This infection had caused her bacterial mastitis and appropriate antibiotics were given. This is very unusual and it was likely confounded by her extreme engorgement and sudden high volume of milk.
Mastitis can also be caused by an imbalance or dysbiosis to the microbiome. The entero-mammary pathway means that microbes can travel from the gut to the breast, meaning that our gut microbiome can affect our breasts. While lots of research is still needed, some studies suggest taking probiotics for mastitis.
My second client this week with mastitis had a large oversupply of breastmilk. Although this may not sound like a problem, it actually is. Mums who hyper lactate are more at risk for recurrent mastitis and often have full uncomfortable breasts alongside a fussy unhappy baby. This condition can be very challenging and needs skilled support to gently bring down their milk supply so that everyone can feel a little better.
All mastitis is unpleasant and I would suggest everyone that has had it works with a breastfeeding specialist, IBCLC, to work out what caused it in the first place.